PANS and PANDAS Syndrome
PANDAS and PANS— Psychoeducation
The information on this page is provided for psychoeducation only. PANS and PANDAS are medical conditions that require diagnosis and treatment by a medical practitioner. Clinicians at this clinic do not diagnose or treat PANS or PANDAS. Our psychologists can offer psychological support and psychoeducation to families, and our nutritionist or dietitian may provide nutritional support where clinically indicated. We are able to refer to medical practitioners who can diagnose and treat these conditions.
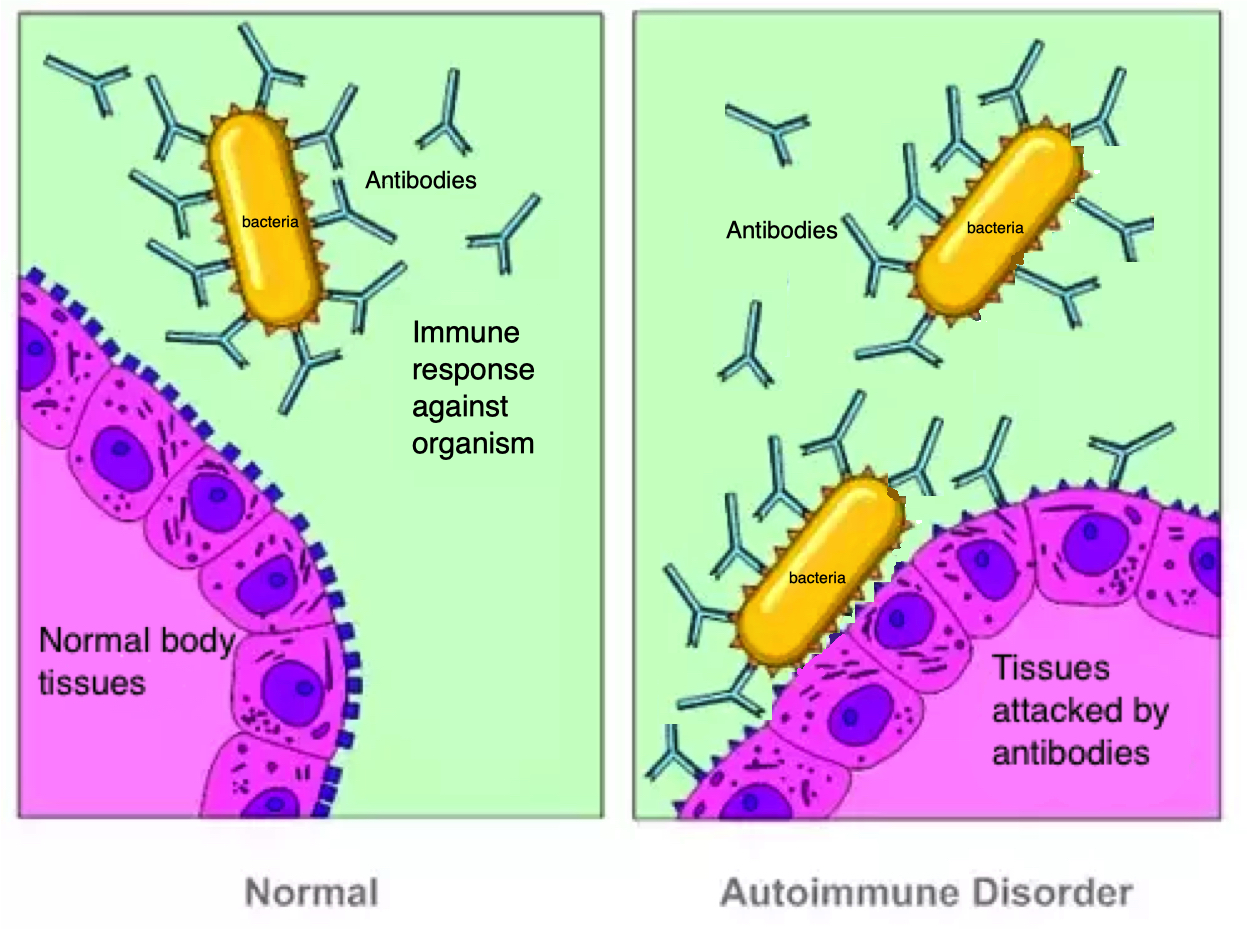
PANDAS (Paediatric Autoimmune Neuropsychiatric Disorders Associated with Streptococcal infections) is a medical diagnosis for children who develop a sudden onset of neuropsychiatric symptoms — such as tics or obsessive-compulsive behaviours — following infection with Group A beta-haemolytic Streptococcus, the bacteria responsible for strep throat and scarlet fever. In genetically predisposed children, the immune response to the infection may mistakenly target structures in the brain through a process called molecular mimicry, producing symptoms that can include tics, OCD behaviours, anxiety, behavioural regression, and cognitive inflexibility (Europe PMC; Taylor & Francis; MDPI, 2024).
PANS (Paediatric Acute-onset Neuropsychiatric Syndrome) is a broader diagnosis encompassing all cases of sudden-onset OCD or severely restricted food intake, regardless of the specific infectious or non-infectious trigger. A PANS diagnosis additionally requires at least two further cognitive, behavioural or mood symptoms such as irritability, anxiety or depression (Journal of Child and Adolescent Psychopharmacology).
Both conditions require medical diagnosis. If you are concerned that your child may have PANS or PANDAS, please consult your GP or paediatrician in the first instance.
Treatment for PANDAS and PANS

Treatment for PANS and PANDAS is managed by medical practitioners. For PANDAS, antibiotics may address the underlying infection, though neuropsychiatric symptoms arise from immune activity rather than the bacteria itself, meaning antibiotic treatment may not immediately resolve behavioural or psychiatric symptoms. Behavioural interventions, psychological therapy and supportive care are established components of management. Decisions about treatment, including the use of long-term antibiotics, should be made on an individualised basis with a treating medical practitioner (MDPI, 2022).
Where psychological support is sought, our psychologists can assist families with psychoeducation and coping strategies. Nutritional support may also be considered where clinically indicated.
Updated on 26/02/2026 by: Dr Jacques Duff- BA Psych; Grad Dip Applied Psychology PhD; MAPS
Reviewed on: 05/03/2026 by: Bernard Ferriere- Clinical Psychologist; BA; Grad Dip Applied Psychology; Dip Clinical Hypnosis; MAPS